






Поскольку чувство зуда является полностью субъективным ощущением, задачей дерматолога становится не только как можно более точное изучение жалоб больного, но и понимание объективных механизмов зуда... об этом и поговорим






This page combines the scientific theory of the diversity of cellular relationships in the skin, the history of the idea, the monograph "Phenotypic Dermatology" atlas "Dermatovenerology: observations in photographs", information about publications, patents, research, technologies, responses to criticism and prospects for the development of phenotypic dermatology.
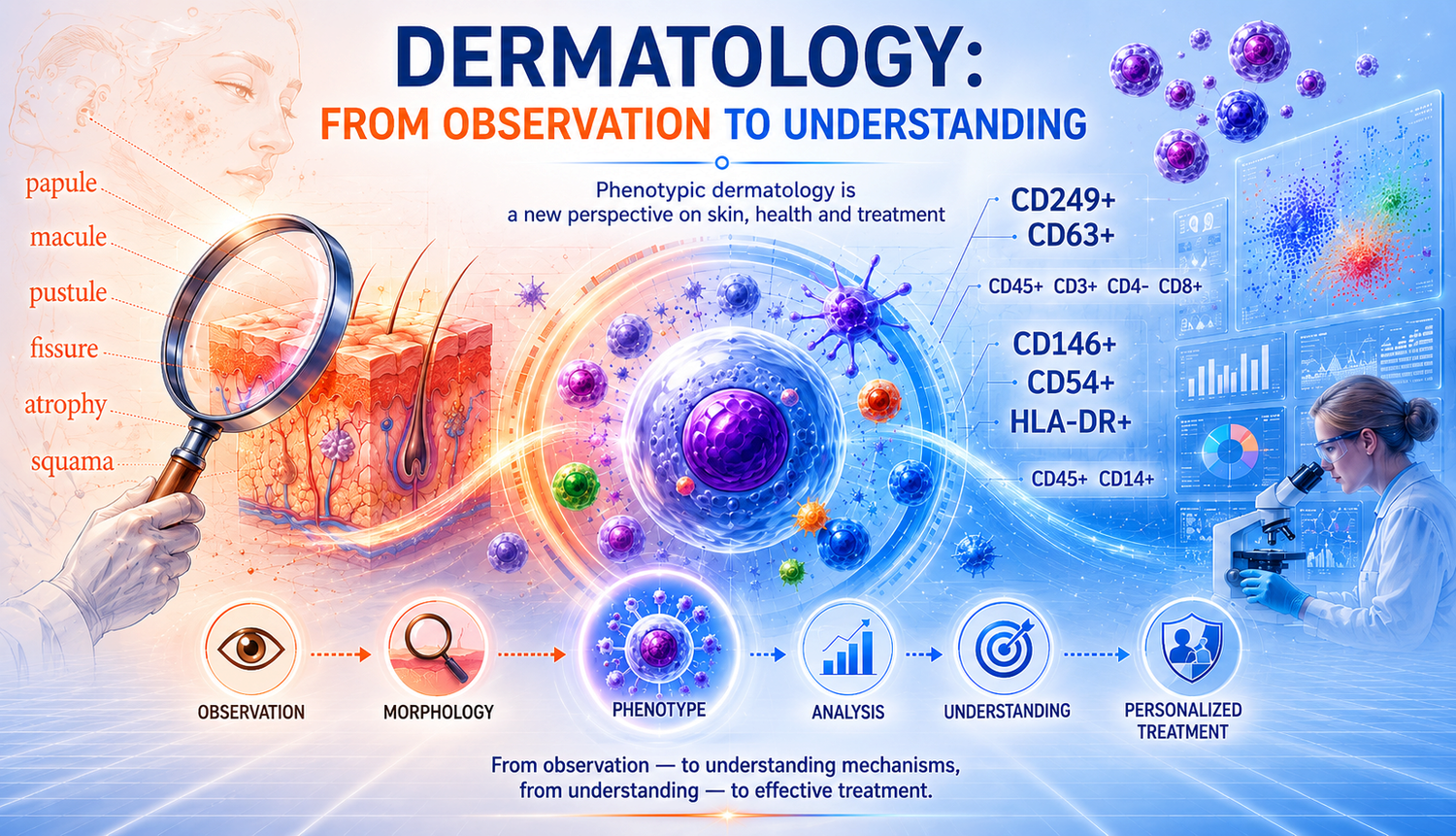
Phenotypic dermatology is a field of dermatology that considers the phenotype of skin cells as the basic unit of analysis of the pathological process.
Unlike the traditional morphological approach, phenotypic dermatology focuses on the objective study of the subpopulation composition of skin cells, their functional state and intercellular interactions. This is a look inside the skin, at the level of its cells, to their phenotypes and complex intercellular relationships. Here, the unit of analysis is not the morphological element, but the living cell and its place in the tissue orchestra.
Based on the flow cytometry method and the technologies I have developed, it is possible to objectively measure what previously escaped the eye: the composition of subpopulations of skin cells, their dynamics, the degree of interaction and response. These data are combined into a "skin cytoimmunogram" — a skin map that allows you to prescribe accurate, personalized treatment. This opens the way to a more scientific, accurate and honest dermatology of the future.
The path I chose required going beyond the usual clinical logic. I had to turn to conceptual analysis to find a language to describe new phenomena. After all, it is the diversity of intercellular relationships that gives rise to properties that determine skin health or disease. Delving into this diversity takes dermatology to a new level — the phenotypic one. He allows you to say,
"What is there is measurable, even if the doctor doesn't see it."
Arguing that the phenotype of a subpopulation of cells becomes the "unit of measurement" of the skin condition, I am aware of the radical message, but at the same time the need for such a sharp turn in the diagnostic thinking of a dermatologist, since it opens up a wide class of research tasks and new therapeutic possibilities. How can you resist?
Phenotypic dermatology is a new scientific paradigm in which the diagnosis and treatment of skin diseases are based not on visual signs, but on objective characteristics of cellular phenotypes and their interactions.
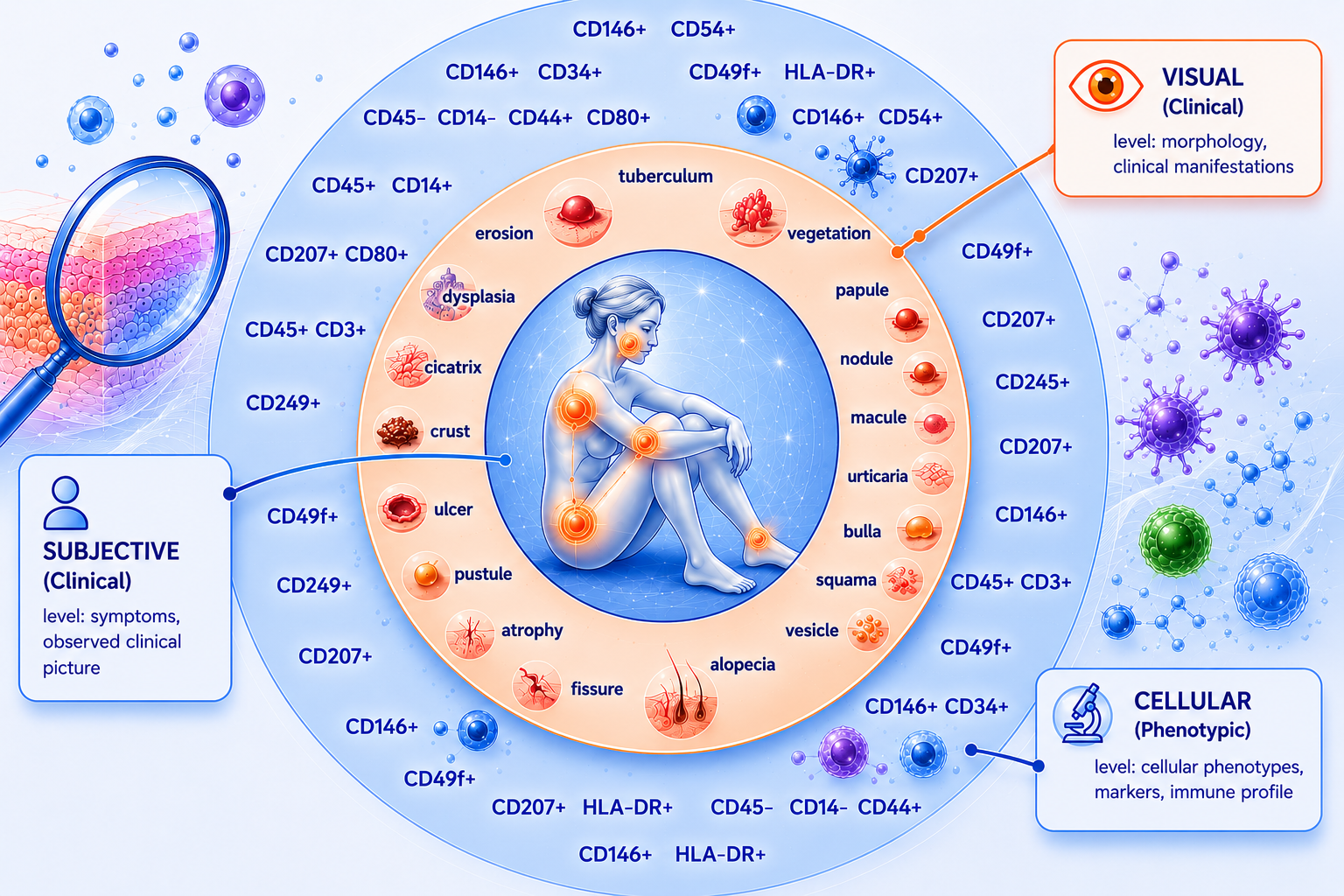
Unlike classical dermatology, which is based on the description of the morphological elements of the rash, phenotypic dermatology considers the skin as a dynamic system of subpopulations of cells and the immune microenvironment.
The methodological basis is flow cytometry and the skin cytoimmunogram method developed by me, a method for obtaining and analyzing viable cell suspensions that allows us to determine the subpopulation composition of cells, their phenotypes and functional state. This approach makes it possible to move from subjective diagnosis to a precision (accurate and measurable) assessment of skin condition, where the "unit of measurement" is the cell phenotype rather than the clinical symptom.
Phenotypic dermatology combines the ideas of cell biology, immunology and systems analysis, creating the basis for personalized therapy.
It opens the way to predicting the course of diseases, choosing optimal treatment methods, and monitoring the effectiveness of interventions. Thus, the theory forms the foundation for a new, scientifically based and measurable dermatology – the dermatology of phenotypes.

This is how phenotypic dermatology appeared, as a prerequisite for the need to go beyond the visual-descriptive stage and move to the phenotypic level.
This transition opens up new horizons for doctors and researchers: from more accurate diagnosis to predictable treatment results.
Surprisingly, looking back, I understand more and more clearly.: this theory was not created in conditions of abundance. She didn't have enough time, because life demanded something else. She didn't have enough resources, because each experiment literally had to be paid for by her own belief in its necessity. She had no support, because new things are rarely accepted right away. And, perhaps most importantly, she had no guarantee of her own rightness.
Phenotypic dermatology was formed in conditions of scarcity. The scarcity of everything.
And it is precisely this circumstance, which could be considered a weakness, that eventually turned out to be its main feature. The deficit did not allow mistakes to be made without consequences. The shortage left no room for excess. The deficit did not allow for redundancy – neither in concepts, nor in interpretations, nor in conclusions.
Each statement had to be verified not only by experiment, but also by internal consistency. Every decision had to be justified not theoretically, but practically. Every hypothesis had to be questioned.… First of all, my own.
Under these conditions, the theory was not constructed. She was being selected. Everything superfluous was taken away. Everything that could not withstand the pressure of reality was discarded. The only thing that remained was what continued to work, no matter what. And that is why today I increasingly think that it is more correct to talk not about the creation of this theory, but about its formation under conditions of selection.
Phenotypic dermatology is not a product of an excessive scientific environment. This is the result of constraints in which only what is necessary survives. This is a theory that initially had no room for error.
After 30 years of clinical practice as a dermatologist, I dared to say out loud: The usual diagnosis based on rashes and morphological elements no longer meets the demands of the time. It traps the doctor in subjectivity: "a dermatologist treats what he sees, and sees what he knows." But sore skin is much more than a collection of spots, papules, plaques, and other rash elements.
The book is based on an officially registered scientific discovery: a method of separating skin cells while preserving their viability. Its use is already yielding specific clinical results, which are described in detail in the monograph.
This publication is aimed at dermatologists, from students to professors. First, it can become the basis for future research. The second is a demonstration of how old problems are solved in a new way, when the usual morphology gives way to the phenotype and function of skin cells.
Buy the printed version
At the same time, I would like to highlight the book, which has become a prerequisite in the scientific search from observation to understanding. In fact, both books present a consistent ontology of a new type of dermatology, in which the stages are clearly traced.:
 1. Dermatovenerology: observations in photos about:
1. Dermatovenerology: observations in photos about:
→ Observation
→ morphology
→ language of the symptom
 2 . Phenotypic dermatology pro:
2 . Phenotypic dermatology pro:
→ discrimination
→ the cell
→ language of explanation
 |
 |
 |
 |
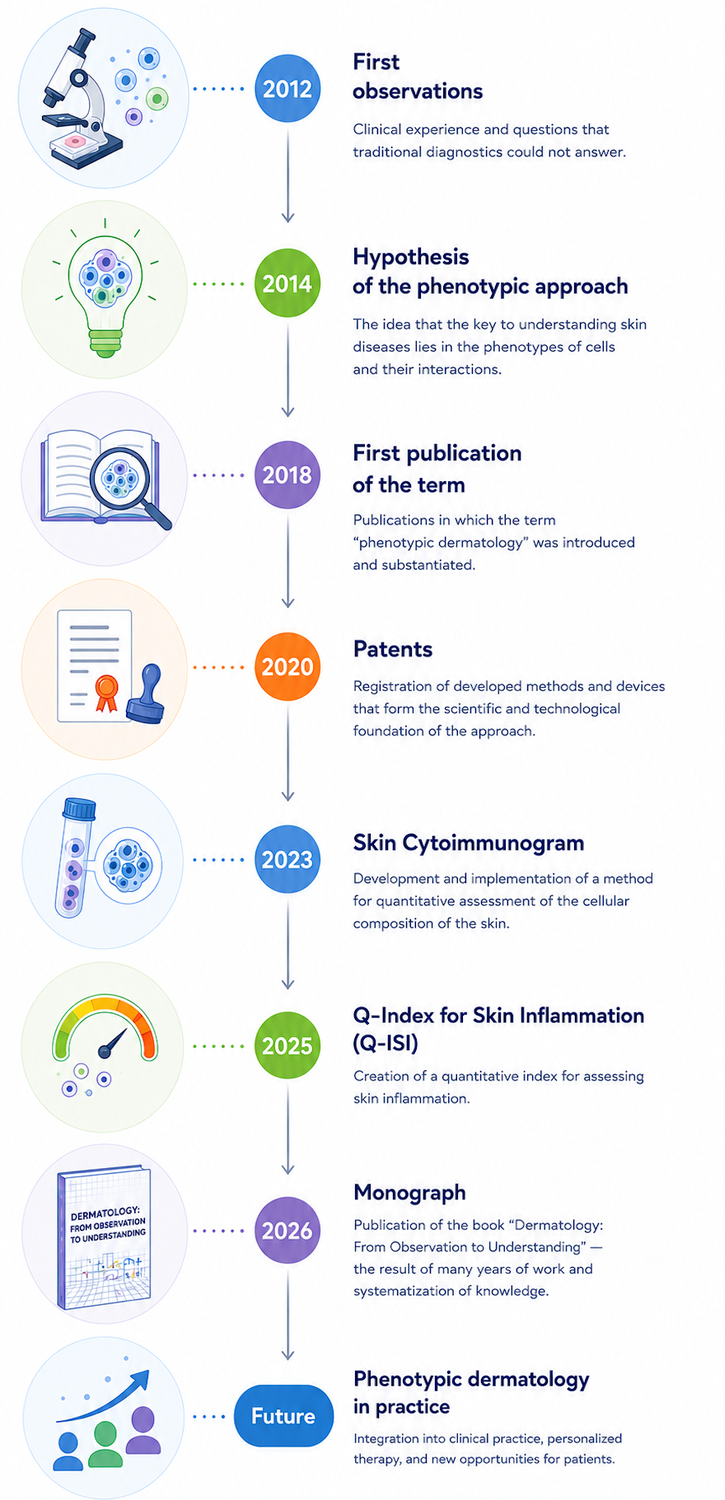
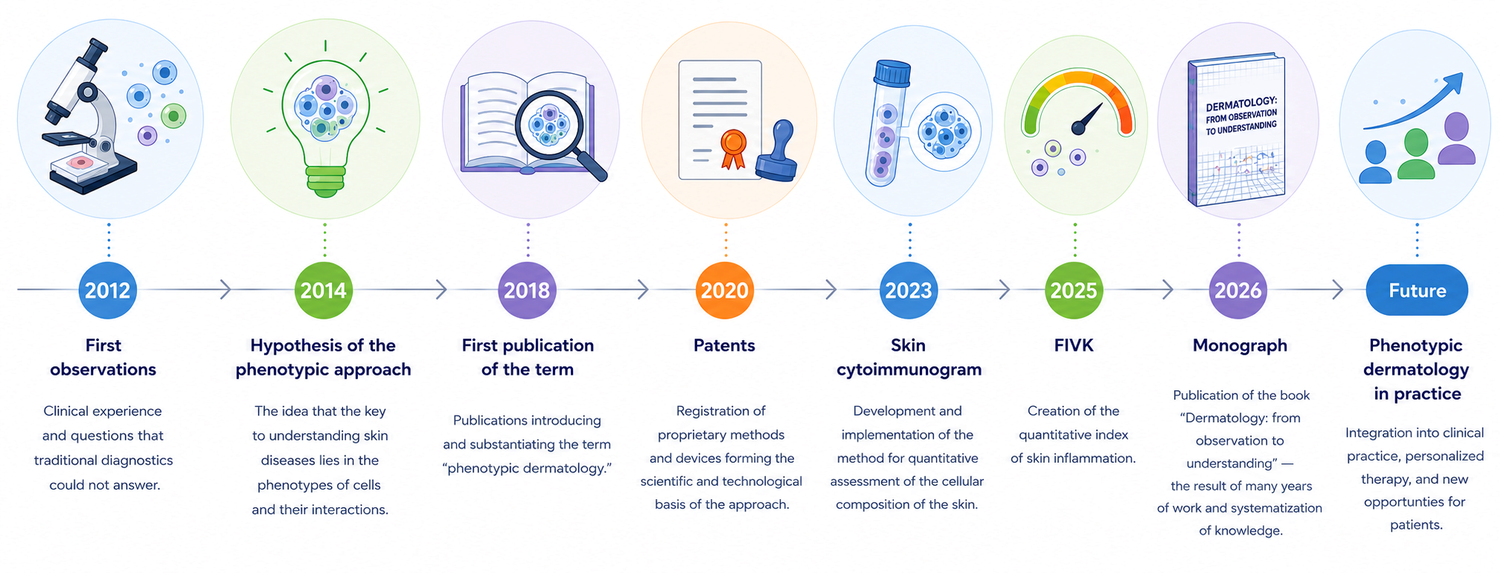
More than 14 years of research
The theory was formed as a result of many years of observations, experimental work and the search for objective methods for assessing the condition of the skin. During this time, the scientific and technological base was formed, which made it possible to move from hypotheses to measurable parameters.
Development of methods for obtaining viable skin cells
One of the key stages was the creation of a technology for isolating a viable heterogeneous population of skin cells while maintaining their functional activity. This opened up the possibility of direct investigation of the cellular composition of the skin by flow cytometry.
Creation of a skin cytoimmunogram
Based on the obtained cell suspensions, the skin cytoimmunogram method was developed — a method for quantifying the subpopulation composition of cells, their phenotypes and functional state. The method allows an objective investigation of processes that were previously unavailable for direct measurement.
The patent foundation
The developed technologies are protected by patents of the Russian Federation. The patent portfolio covers methods for obtaining and analyzing skin cells, devices for activating reparative processes, as well as regenerative therapy technologies.
Clinical trials
The developed methods were used in the study of various pathological conditions of the skin, processes of inflammation, regeneration and wound healing. The data obtained formed the basis for the further development of the phenotypic approach to diagnosis and therapy.
Scientific publications
The research results are presented in scientific articles, reports, abstracts, patents, and the monograph "Dermatology: from Observation to Understanding." The publication activity reflects the gradual formation and development of the concept of phenotypic dermatology.
Phenotypic dermatology relies on experimental data, objective measurement technologies, and long-term research practice, combining advances in cell biology, immunology, and clinical dermatology.
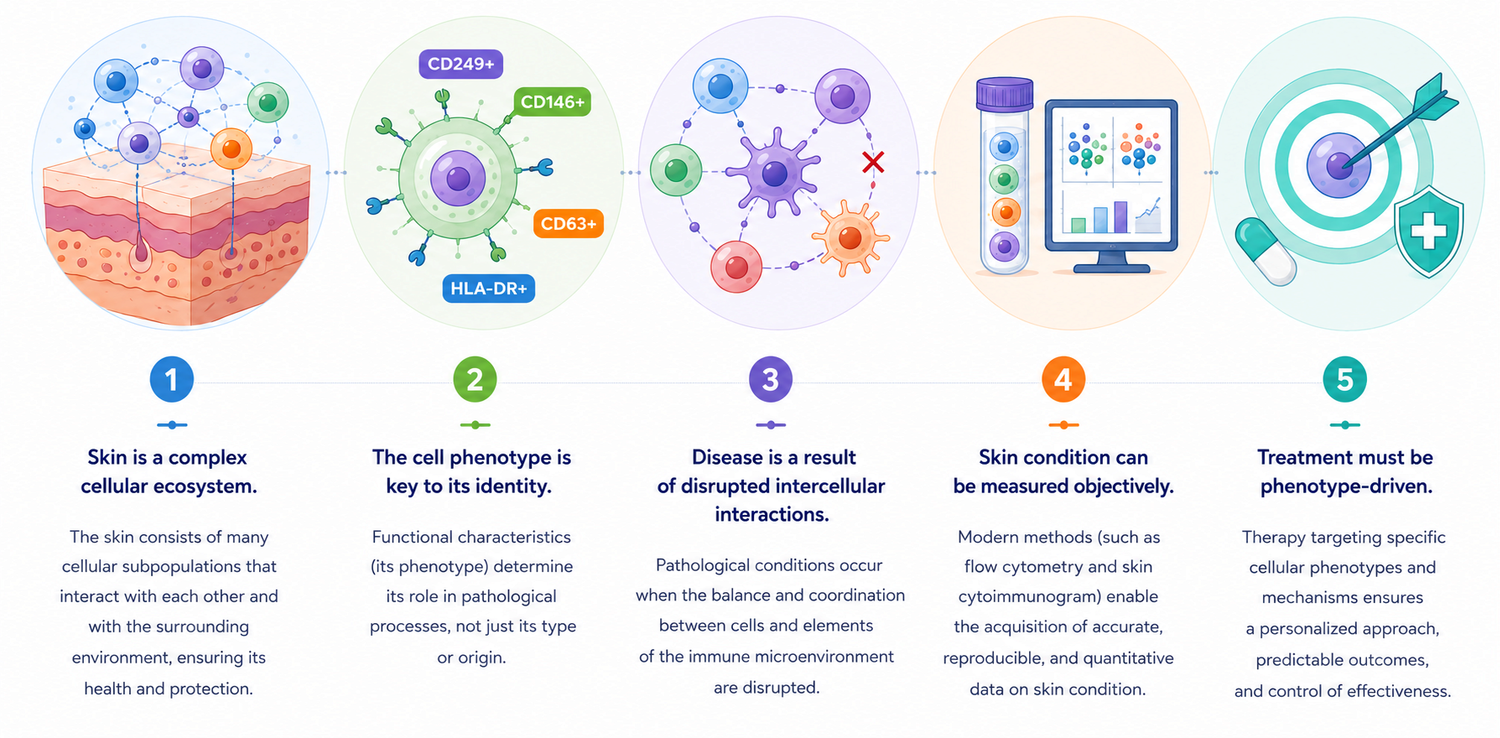
Skin is a complex cellular ecosystem
The skin is not a set of individual cells, but a complex system of interconnected cellular subpopulations and elements of the microenvironment that continuously interact with each other to maintain its structure and functions.
The phenotype of a cell is more important than its type
The behavior of a cell is determined not only by its origin, but also by its current functional state. It is the phenotype that reflects the activity of the cell, its role in the pathological process and participation in intercellular interactions.
The disease is the result of a violation of intercellular interactions
Many skin diseases do not occur due to changes in individual cells, but due to a disruption in communication between cell populations and elements of the immune microenvironment.
The condition of the skin can be measured objectively
Modern methods of cell analysis make it possible to obtain quantitative data on the composition of skin cells, their phenotypes and functional state, transferring diagnostics from the field of subjective observations to the field of measurable indicators.
Treatment should be phenotypically based
The choice of therapy should take into account not only the clinical manifestations of the disease, but also the characteristics of the cellular phenotypes underlying the pathological process, which opens the way to personalized treatment.
 Presidium of the X Conference of Immunologists of the Urals with international participation (Tyumen, 2012): E.A. Kashuba, Rector of the Tyumen State Medical Academy, Professor, Doctor of Medicine; N.S. Brynza, First Deputy Director of the Tyumen Region Department of Health, Head of the Department of Health Organization and Public Health of the Tyumen State Medical Academy, Professor, MD; V.A. Chereshnev, Academician of the Russian Academy of Sciences and the Russian Academy of Medical Sciences, President of the Russian Scientific Society of Immunologists and the Ural Society of Immunologists, Allergologists and Immunorehabilitologists, Director of the Institute of Immunology and Physiology of the Ural Branch of the Russian Academy of Sciences, presChairman of the Committee of the State Duma of the Federal Assembly of the Russian Federation on Science and High-tech Technologies, Professor, Doctor of Medical Sciences; V.P. Melnikov, Academician of the Russian Academy of Sciences, Director of the Tyumen Scientific Center of the Siberian Branch of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences; I.A. Tuzankina, Scientific Secretary of the Institute of Immunology and Physiology of the Ural Branch of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences; A.A. Yarilin, Professor, Doctor of Medical Sciences
Presidium of the X Conference of Immunologists of the Urals with international participation (Tyumen, 2012): E.A. Kashuba, Rector of the Tyumen State Medical Academy, Professor, Doctor of Medicine; N.S. Brynza, First Deputy Director of the Tyumen Region Department of Health, Head of the Department of Health Organization and Public Health of the Tyumen State Medical Academy, Professor, MD; V.A. Chereshnev, Academician of the Russian Academy of Sciences and the Russian Academy of Medical Sciences, President of the Russian Scientific Society of Immunologists and the Ural Society of Immunologists, Allergologists and Immunorehabilitologists, Director of the Institute of Immunology and Physiology of the Ural Branch of the Russian Academy of Sciences, presChairman of the Committee of the State Duma of the Federal Assembly of the Russian Federation on Science and High-tech Technologies, Professor, Doctor of Medical Sciences; V.P. Melnikov, Academician of the Russian Academy of Sciences, Director of the Tyumen Scientific Center of the Siberian Branch of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences; I.A. Tuzankina, Scientific Secretary of the Institute of Immunology and Physiology of the Ural Branch of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences; A.A. Yarilin, Professor, Doctor of Medical Sciences
Over the years of working on the theory, I have received a number of feedback and comments. I consider them an important part of its development. Criticism allows us to see not only the weaknesses of the new model, but also the limits of its perception within the existing scientific paradigm. Below are some typical remarks.
____________________
An analysis of such comments shows that the main tension does not arise at the level of data, methods, or results. It arises at the level of language and initial assumptions.
On the one hand, there is an established system of concepts based on fixed classifications and traditional diagnostic approaches.
On the other hand, phenotypic dermatology offers a different level of description — to consider the skin as a dynamic system of phenotypes subject to quantitative and functional assessment.
In such circumstances, criticism becomes not only a mechanism for testing a new idea, but also an indicator of the boundaries of the current scientific model.
Therefore, I consider the presented remarks not as an obstacle, but as an important part of the process of theory formation.
Perhaps one of the signs of a truly new model is that it raises doubts at first because it offers a different way of understanding.
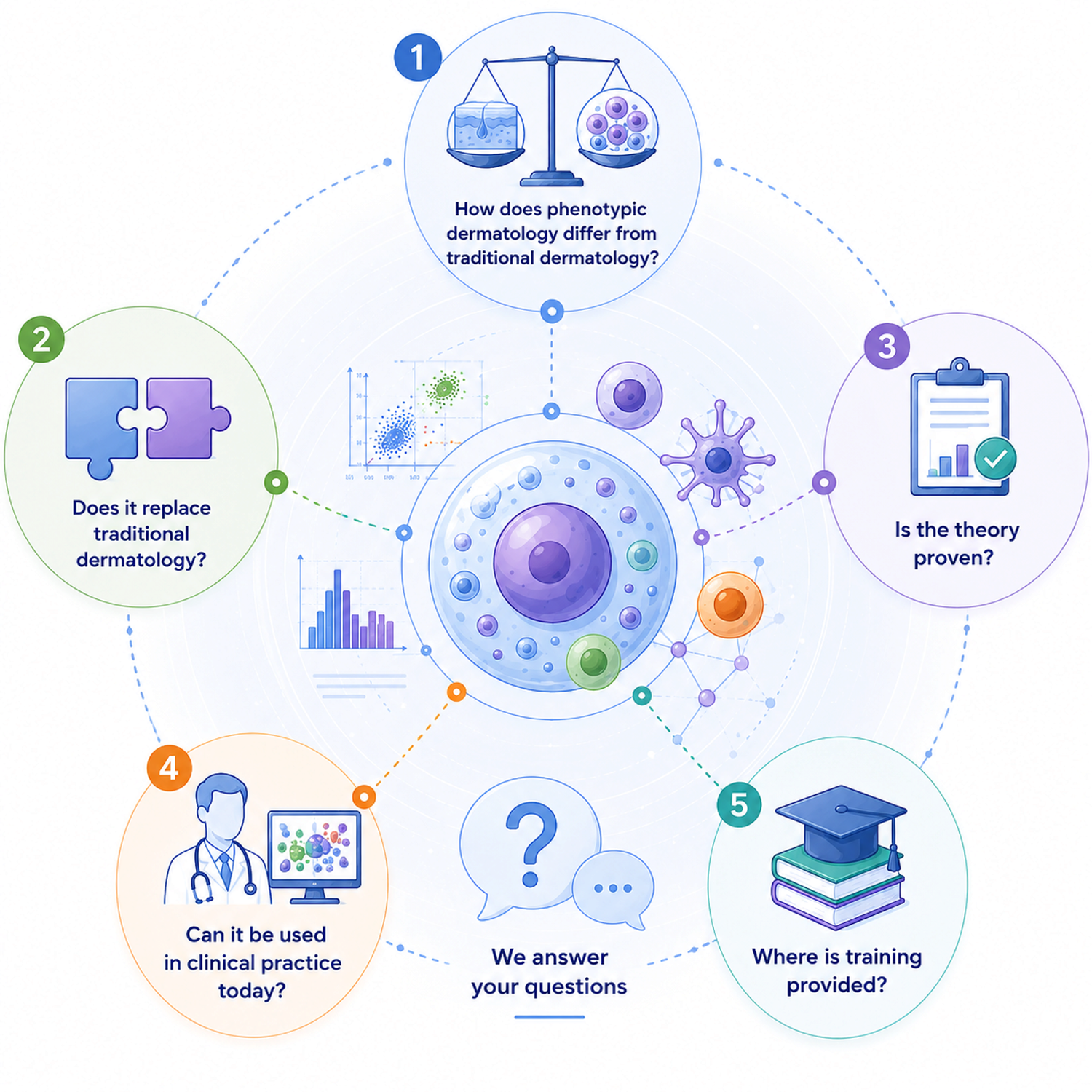
How does phenotypic dermatology differ from classical dermatology?
Classical dermatology mainly relies on a visual assessment of the skin and a description of the morphological elements of the rash. Phenotypic dermatology complements this approach with the study of the cellular composition of the skin, cell phenotypes and their interactions, allowing us to move from observation to objective measurement of the processes underlying the disease.
Does it replace traditional dermatology?
No. Phenotypic dermatology is not opposed to classical dermatology, but develops it. Clinical examination, the doctor's experience and morphological diagnostics retain their importance, but are complemented by modern methods of objective analysis of the skin condition.
Is the theory proven?
The theory is based on many years of research, patents, the development of a method for obtaining viable skin cells, skin cytoimmunograms, and other technologies. Its provisions continue to be developed and verified in scientific and clinical research.
Is it possible to use it in practice today?
Yes. Certain technologies of phenotypic dermatology are already used in scientific work, research and solving practical problems. As methods evolve and data accumulates, the scope of their application will expand.
Where is the training conducted?
Individual technologies and concepts of phenotypic dermatology are taught through educational programs, research projects, publications, and specialized events. Information about the available training formats is published on this website.
What is the "unit of measurement" in phenotypic dermatology?
In phenotypic dermatology, the phenotype of a subpopulation of skin cells becomes the main unit of analysis — a set of its functional characteristics that determine the role of the cell in the norm and in the disease. It is the phenotype that allows us to move from describing the symptoms to understanding the mechanisms of the pathological process.
Why is this important to the patient?
Because treatment should be based not only on what the doctor sees, but also on what is happening in the skin at the cellular level. This approach opens up opportunities for more accurate diagnosis, personalized therapy, and an objective assessment of treatment outcomes.
What has changed for you personally?
This theory has changed me too. If earlier I was looking for answers in symptoms (this is well shown in the first book), today I am looking for them in the relationships between cells. If earlier, for me as a doctor, the disease looked like a set of signs, now I see it as a violation of communication within a living system.
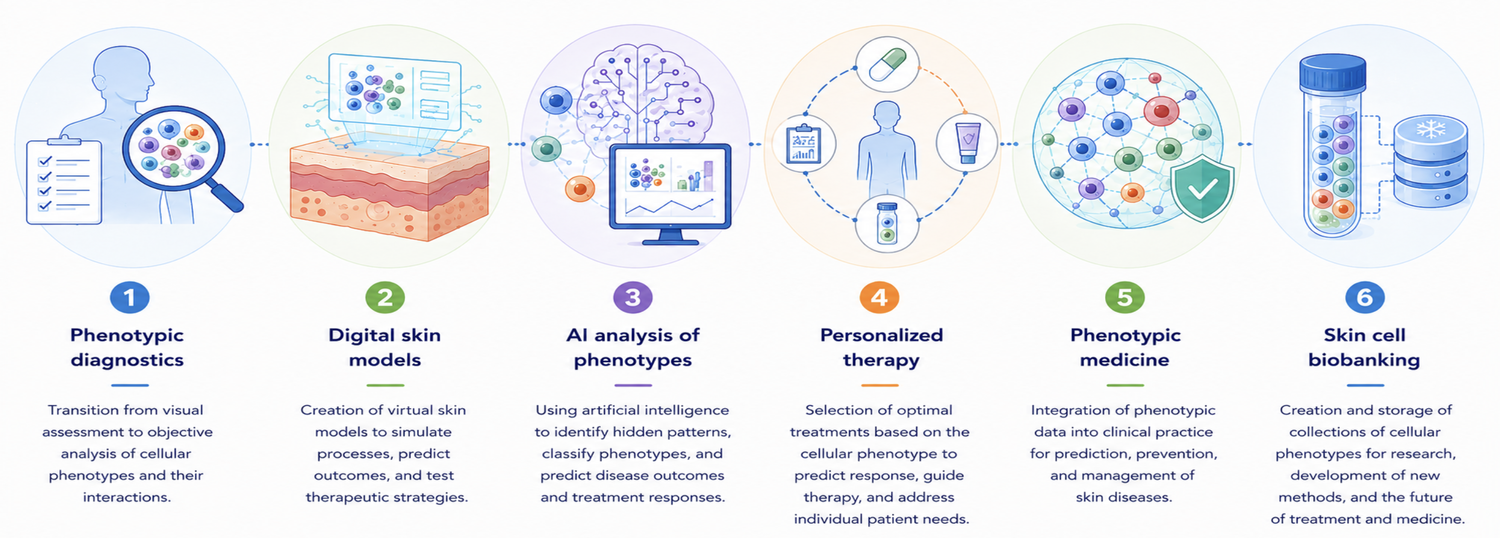
Phenotypic diagnosis
The transition from visual assessment of the skin to an objective analysis of cellular phenotypes and their interactions. This approach allows us to better understand the mechanisms of the disease and identify pathological processes even before the appearance of pronounced clinical manifestations.
Digital skin models
Creation of virtual skin models combining data on cellular composition, phenotypes and intercellular interactions. Such models can be used to predict the course of diseases and evaluate the effectiveness of various treatment methods.
AI analysis of phenotypes
Using artificial intelligence technologies to process large amounts of cellular data. Algorithms are able to identify hidden patterns, classify phenotypes, and help doctors make more accurate diagnostic and therapeutic decisions.
Personalized therapy
Selection of treatment based on the individual characteristics of the cellular microenvironment of the patient. The goal is not only to eliminate the symptoms, but also to influence the specific mechanisms of the disease underlying the pathological process.
Phenotypic medicine
A new stage in the development of medicine, in which diagnosis, prognosis and treatment are based on an objective analysis of cellular phenotypes. This approach is able to combine the achievements of cell biology, immunology, bioinformatics and clinical practice.
Biobanking of skin cells
Creation of systematic collections of skin cells and their phenotypes for scientific research, development of new diagnostic and therapeutic methods. Biobanks form the basis for the accumulation of knowledge and the development of personalized medicine of the future.
"If the transition from observation to understanding has really taken place, then the next step is inevitable — understanding must become manageable."
Sergey Goltsov
is the author of the theory of phenotypic dermatology
Поскольку чувство зуда является полностью субъективным ощущением, задачей дерматолога становится не только как можно более точное изучение жалоб больного, но и понимание объективных механизмов зуда... об этом и поговорим

Conversation on Facebook:
– Where are you?
– Travelling.
– Where this time?
– Where cannibals live.
– ...How are you?
– All parts of my body still belong to me!:)
Seems funny? Click the "like" button. Somebody will say – it can’t be true, what cannibals these days?! A year later after we spent 3 weeks in company with true cannibals as participants of the expedition "Live Parallel in Papua New Guinea", I can hardly believe it myself. Shall we remember it together?
Что это? What’s happened?
It’s incredible! Es increíble! – хотелось прокричать на всех языках каждый миг этого дня, потому как поверить в случившееся сложно.

Even to the horrors of war, the doctor gets used to much faster than an ordinary person, as well as soldiers, after two or three weeks already much without noticing and assessing what is happening, as a matter of course. What can we say about the events taking place during the expedition, when the phenomenon recorded by the photo may contain a different depth of meaning, often understood only after some time. The expedition Live Parallel, organized by Professor A. G. Teslinov in Peru and Bolivia and ended 2 months ago, was not an exception for me. Read more...